A direct look at the large bowel — with the option to act in the same sitting.
A colonoscopy uses a slim, flexible camera — about the thickness of a finger — to examine the entire large bowel, from the rectum to the join with the small intestine. The camera carries instruments that allow the operator not only to look, but to act: a suspicious polyp seen during the procedure can usually be removed there and then.
This combination of diagnosis and treatment in one sitting is what makes colonoscopy unusual among medical tests. The procedure is performed under conscious sedation by an anaesthetist; you remain breathing on your own, but you sleep through the examination and remember nothing of it. Most patients are surprised by how unremarkable the experience is.
An OGD (oesophagogastroduodenoscopy, sometimes called a gastroscopy) is the upper counterpart: a slim camera passed through the mouth to examine the oesophagus, stomach and the first part of the small bowel. The two procedures are often combined in a single appointment.
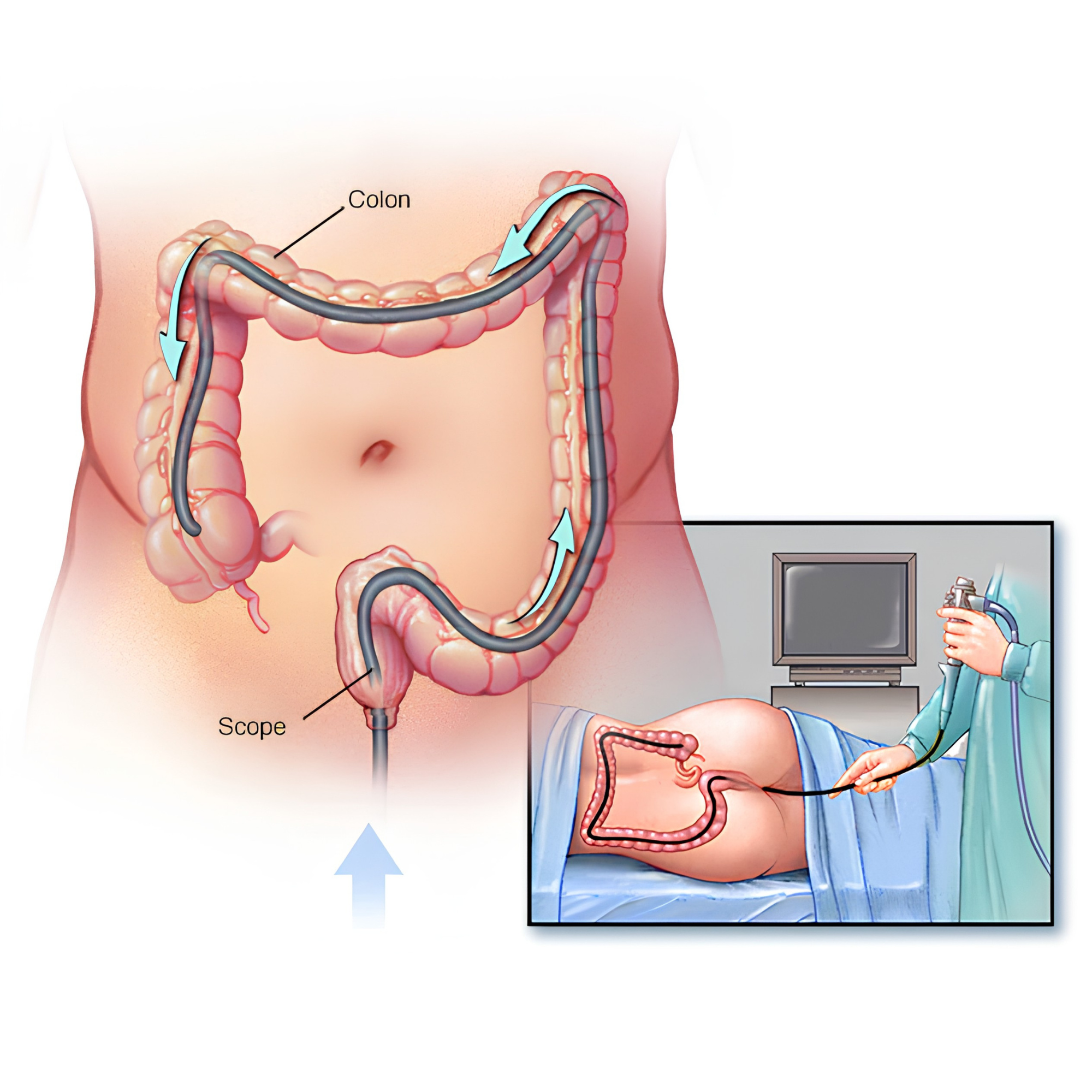
Colonoscopy — the lower-GI scope passes through the large bowel under sedation. The bowel is examined and any polyps removed in the same sitting.
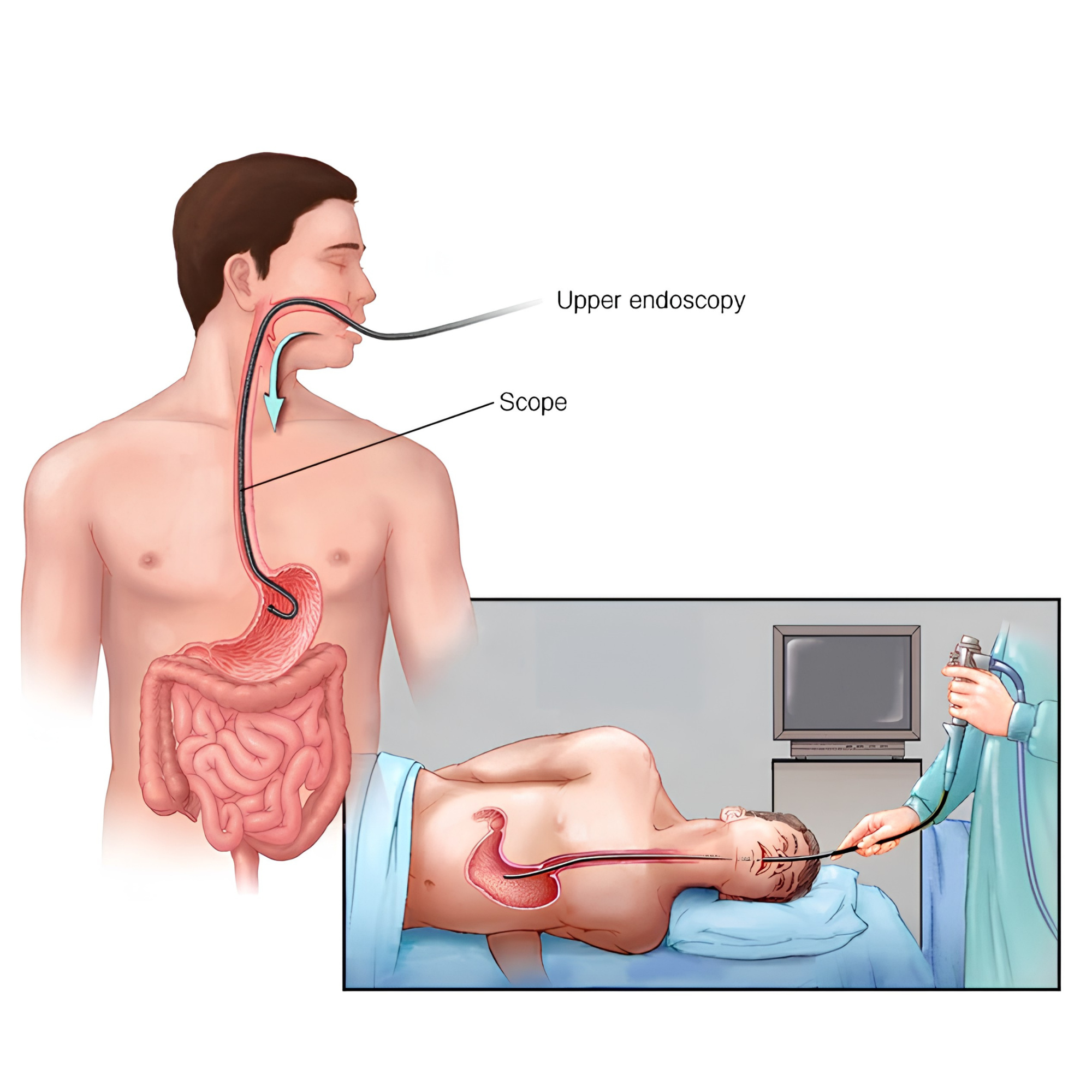
Upper-GI endoscopy (OGD / gastroscopy) — the upper counterpart. A slim scope is passed through the mouth to examine the oesophagus, stomach and duodenum, also under sedation.