Colorectal cancer
The most common cancer in Malaysian men. Found early, it is one of the most curable.
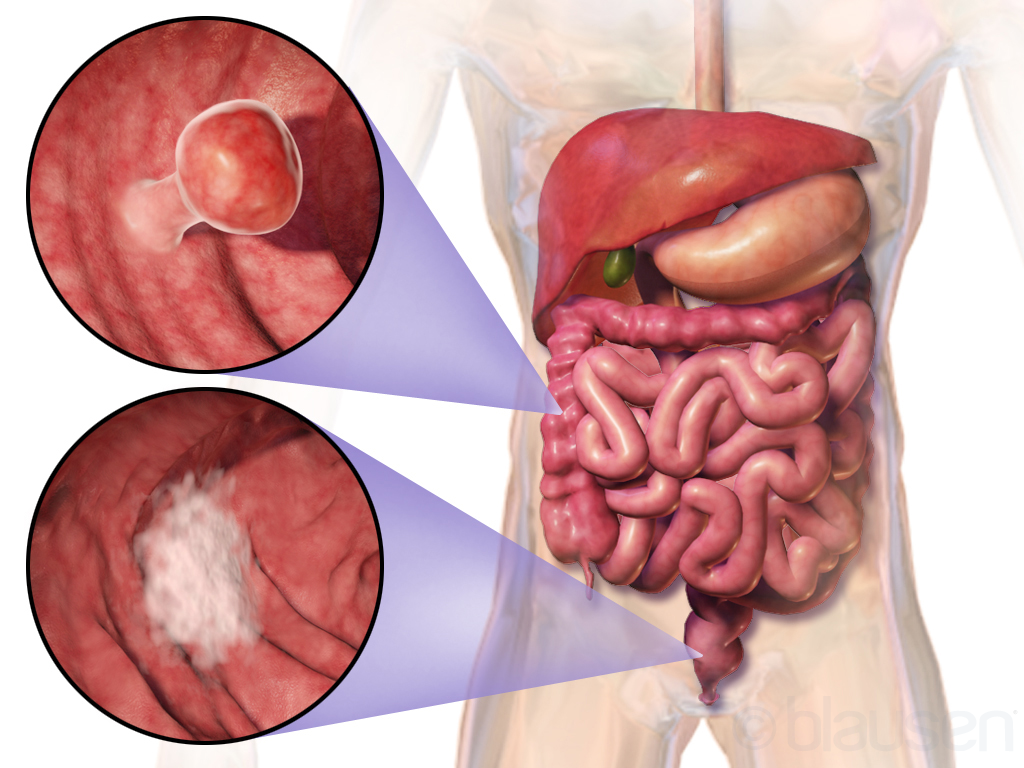
Colorectal cancer develops, in almost all cases, from a small benign growth in the bowel called a polyp. Polyps grow silently and slowly over many years. If they are found early — at colonoscopy — they can be removed in the same sitting and the cancer is prevented before it ever starts. When polyps are not found, a small minority eventually become invasive cancer.
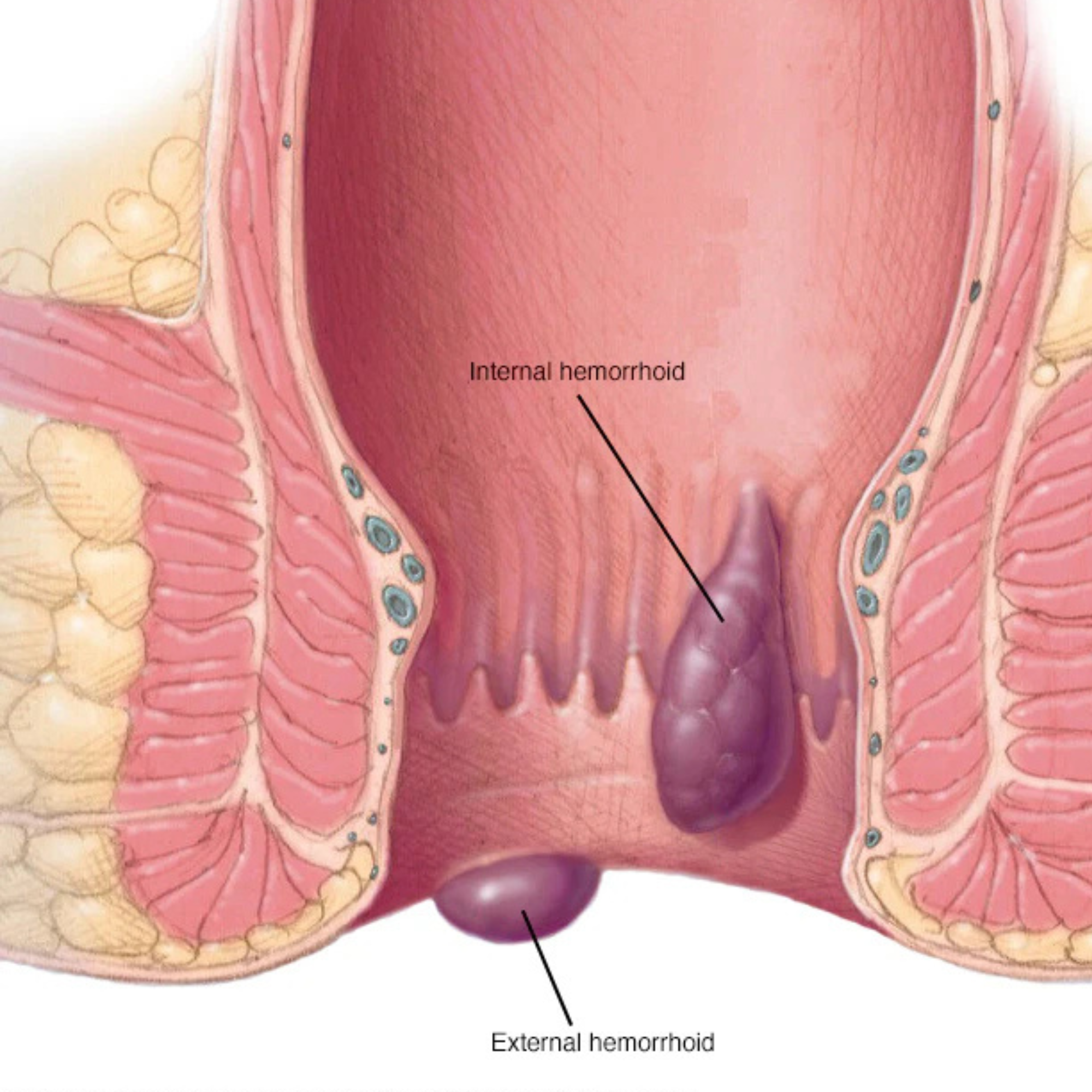
Early colorectal cancer rarely produces dramatic symptoms. Quietly persistent changes are more typical: a change in the shape or frequency of bowel movements, a sense of incomplete emptying, intermittent rectal bleeding (often blamed, wrongly, on haemorrhoids), unexplained iron-deficiency anaemia, or a low-grade abdominal discomfort. Weight loss and severe symptoms tend to appear later — which is why screening matters.
Treatment depends heavily on the stage of disease at diagnosis. Early-stage cancers are often curable with surgery alone, increasingly through minimally invasive keyhole approaches. More advanced cancers are managed with a combined plan — chemotherapy, radiotherapy and surgery — coordinated across a multidisciplinary team. By a long way, the most important variable in outcome is the stage at which it is found.
When to see a specialist
Any new rectal bleeding, a persistent change in bowel habit beyond a few weeks, unexplained tiredness or anaemia, or a family history of bowel cancer. None of these symptoms guarantee cancer — most have benign explanations — but they justify a single consultation to settle the question.