01
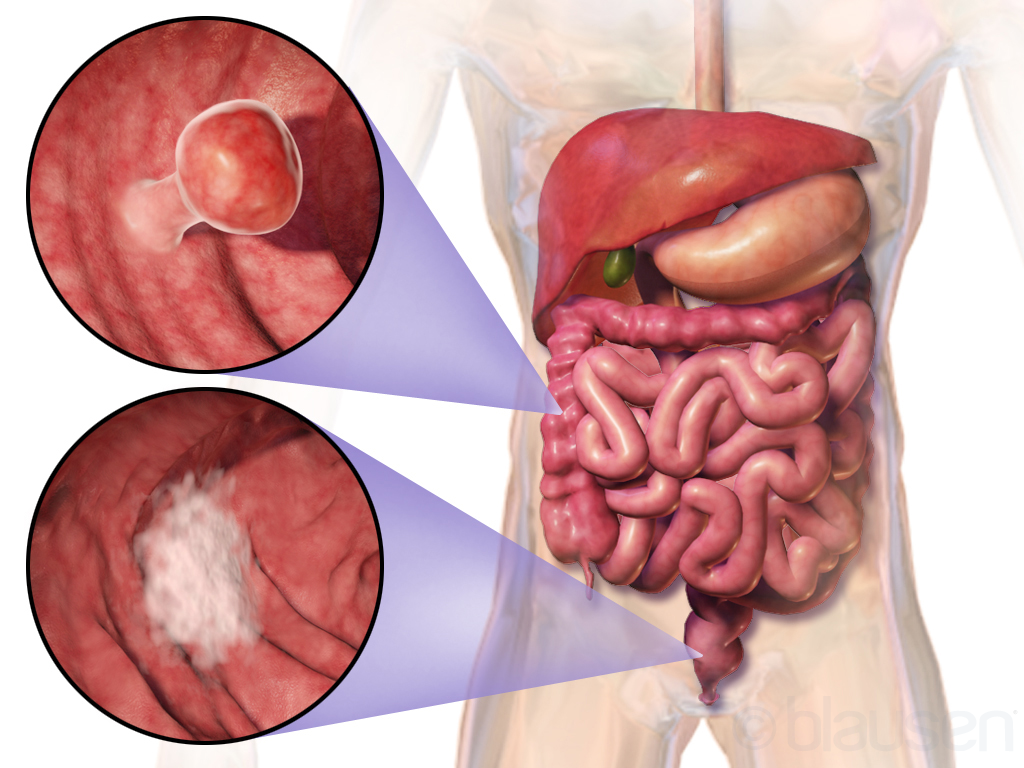
Laparoscopic Colorectal Cancer Surgery
Keyhole bowel resection with full lymph-node clearance.
The keyhole removal of a segment of the bowel containing a cancer, together with its draining lymph nodes. Performed through four or five small abdominal incisions, with one slightly larger cut to deliver the specimen.
The technique reduces post-operative pain, shortens hospital stay to typically four to six days, and allows most patients to return to office work within three to four weeks. The same oncological principles apply as in open surgery — the resection is no less radical because it is performed laparoscopically.